
Rational Use of Ceftriaxone in Necrotizing Fasciitis and Mortality Associated with Bloodstream Infection and Hemorrhagic Bullous Lesions

 , ,
, ,
Abstract
:1. Introduction
2. Results
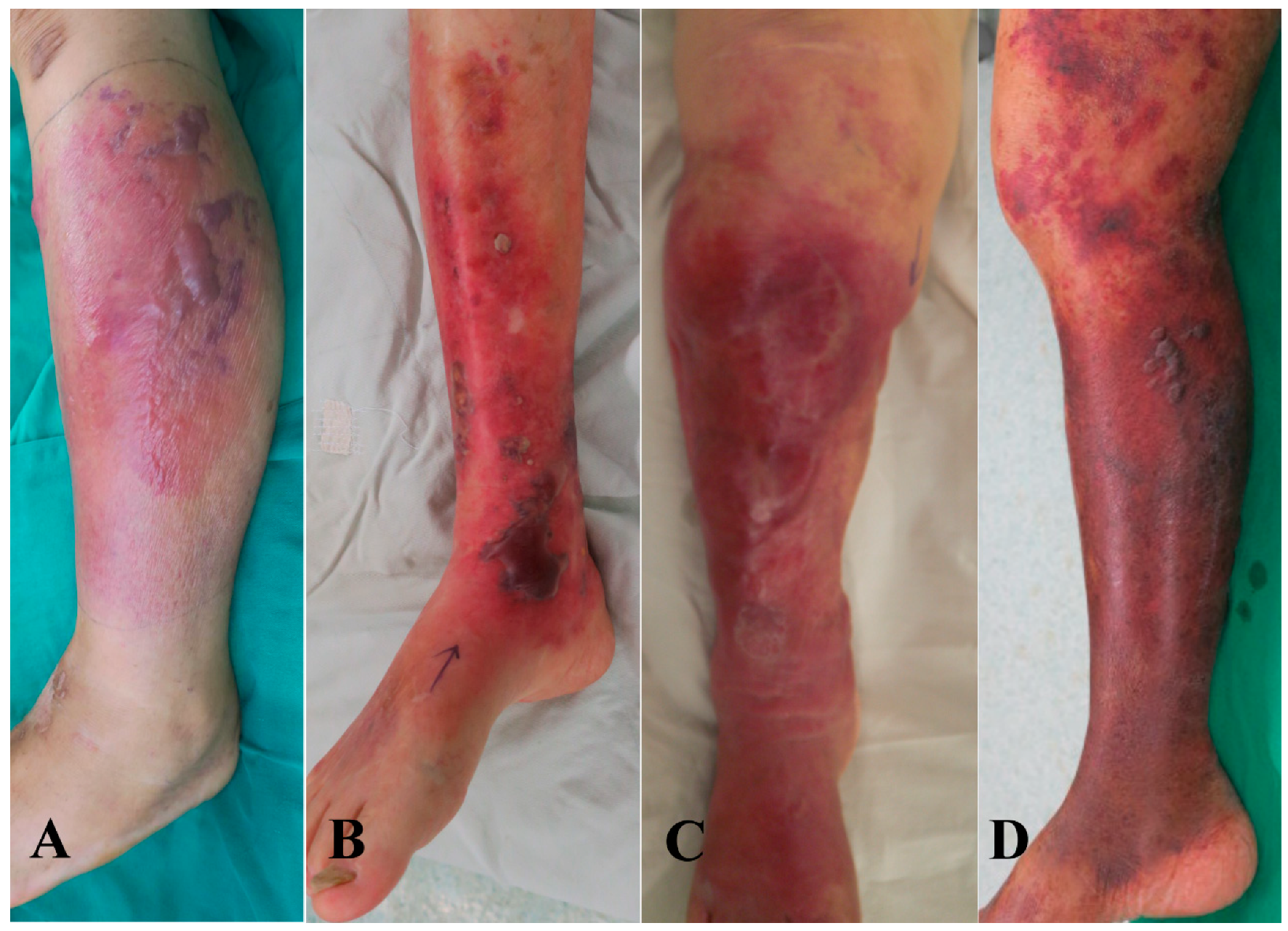
2.1. Microbiological Findings and Hemorrhagic Skin Presentation in NF Patients
2.2. Patient Characteristics in the Gram-Negative Group
2.3. Patient Characteristics in the Gram-Positive Group
2.4. Antibiotic Susceptibility and Resistance of Gram-Negative and Gram-Positive Pathogens
2.5. Comparison of Gram-Negative and Gram-Positive Groups
3. Discussion
4. Materials and Methods
4.1. Patient Selection
4.2. Diagnosis and Treatment Protocol
4.3. Clinical Assessment
4.4. Microbiology Laboratory Procedures
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Wong, C.H.; Chang, H.C.; Pasupathy, S.; Khin, L.W.; Tan, J.L.; Low, C.O. Necrotizing fasciitis: Clinical presentation, microbiology, and determinants of mortality. JBJS 2003, 85A, 1454–1460. [Google Scholar] [CrossRef] [Green Version]
- Fontes, R.A., Jr.; Ogilvie, C.M.; Miclau, T. Necrotizing soft-tissue infections. J. Am. Acad. Orthop. Surg. 2000, 8, 151–158. [Google Scholar] [CrossRef]
- Elliott, D.; Kufera, J.A.; Myers, R.A. The microbiology of necrotizing soft tissue infections. Am. J. Surg. 2000, 179, 361–366. [Google Scholar] [CrossRef]
- Morgan, M.S. Diagnosis and management of necrotising fasciitis: A multiparametric approach. J. Hosp. Infect. 2010, 75, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wong, C.; Tay, Y. Staging of necrotising fasciitis based on the evolving cutaneous features. Int. J. Dermatol. 2007, 46, 1036–1041. [Google Scholar] [CrossRef]
- Kiat, H.J.; Natalie, Y.H.E.; Fatimah, L. Necrotizing fasciitis: How reliable are the cutaneous signs? J. Emerg. Trauma. Shock. 2017, 10, 205–210. [Google Scholar] [PubMed]
- Hsiao, C.T.; Lin, L.J.; Shiao, C.J.; Hsiao, K.Y.; Chen, I.C. Hemorrhagic bullae are not only skin deep. Am. J. Emerg. Med. 2008, 26, 316–319. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.M.; Hsiao, C.T.; Chung, K.J.; Kung, C.T.; Hung, S.C.; Liu, P.P. Hemorrhagic bullae represent an ominous sign for cirrhotic patients. J. Emerg. Med. 2008, 34, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.Y.; Tsai, Y.H.; Kuo, L.T.; Hsu, W.H.; Hsiao, C.T.; Hung, C.H.; Huang, W.Y.; Wu, H.R.; Chuang, H.J.; Li, Y.Y.; et al. Different types of bullae of limbs with necrotizing fasciitis predict different outcome: A prospective study. Infection 2021, 49, 135–144. [Google Scholar] [CrossRef]
- Cohen, L.; Kang, H.; Sochol, K.; Cohen, S.; Ghiassi, A.; Stevanovic, M.; Lefebvre, R. Differentiating upper extremity necrotizing soft tissue infection frome serious cellulitis and abscess. Cureus 2021, 13, e17806. [Google Scholar]
- Fernando, S.M.; Tran, A.; Cheng, W.; Rochwerg, B.; Kyeremanteng, K.; Seely, A.J.; Inaba, K.; Perry, J.J. Necrotizing soft tissue infections: Diagnostic accuracy of physical examination, imaging, and LRINEC score. Ann. Surg. 2019, 269, 58–65. [Google Scholar] [CrossRef]
- Tsai, Y.H.; Hsu, R.W.; Huang, K.C.; Huang, T.J. Laboratory indicators for early detection and surgical treatment of Vibrio necrotizing fasciitis. Clin. Orthop. Relat. Res. 2010, 468, 2230–2237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, Y.H.; Huang, T.Y.; Chen, J.L.; Hsiao, C.T.; Kuo, L.T.; Huang, K.C. Bacteriology and mortality of necrotizing fasciitis in a tertiary coastal hospital with comparing risk indicators of methicillin-resistant Staphylococcus aureus and Vibrio vulnifcus infections: A prospective study. BMC. Infect. Dis. 2021, 21, 771. [Google Scholar] [CrossRef]
- Hsiao, C.T.; Weng, H.H.; Yuan, Y.D.; Chen, C.T.; Chen, I.C. Predictors of mortality in patients with necrotizing fasciitis. Am. J. Emerg. Med. 2008, 26, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.Y.; Peng, K.T.; Hsu, W.H.; Hung, C.H.; Chuang, F.Y.; Tsai, Y.H. Independent Predictors of Mortality for Aeromonas Necrotizing Fasciitis of Limbs: An 18-year Retrospective Study. Sci. Rep. 2020, 10, 7716. [Google Scholar] [CrossRef]
- Tsai, Y.H.; Huang, T.Y.; Kuo, L.T.; Chuang, P.Y.; Hsiao, C.T.; Huang, K.C. Comparison of surgical outcomes and predictors in patients with monomicrobial necrotizing fasciitis caused by Vibrio vulnificus, Aeromonas hydrophila and Aeromonas sobria. Surg. Infect. 2022, 23, 288–297. [Google Scholar] [CrossRef]
- Tsai, Y.H.; Hsu, R.W.W.; Huang, K.C.; Huang, T.J. Comparison of necrotizing fasciitis and sepsis caused by Vibrio vulnificus and Staphylococcus aureus. JBJS 2011, 93, 274–284. [Google Scholar] [CrossRef]
- Tsai, Y.H.; Huang, K.C.; Shen, S.H.; Hsu, W.H.; Peng, K.T.; Huang, T.J. Microbiology and surgical indicators of necrotizing fasciitis in a tertiary hospital of southwest Taiwan. Int. J. Infect. Dis. 2012, 16, e159–e165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevens, D.L.; Bryant, A.E. Necrotizing soft-tissue infections. N. Engl. J. Med. 2017, 377, 2253–2265. [Google Scholar] [CrossRef]
- Pelletier, J.; Gottlieb, M.; Long, B.; Perkins, J.C., Jr. Necrotizing soft tissue infections (NSTI): Pearls and pitfalls for the emergency clinician. J. Emerg. Med. 2022, 62, 480–491. [Google Scholar] [CrossRef] [PubMed]
- Montravers, P.; Snauwaert, A.; Welsch, C. Current guidelines and recommendations for the management of skin and soft tissue infections. Curr. Opin. Infect. Dis. 2016, 29, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Urbina, T.; Razazi, K.; Ourghanlian, C.; Woerther, P.L.; Chosidow, O.; Lepeule, R.; de Prost, N. Antibiotics in Necrotizing Soft Tissue Infections. Antibiotics 2021, 10, 1104. [Google Scholar] [CrossRef]
- Rampal, S.; Ganesan, T.; Sisubalasingam, N.; Neela, V.K.; Tokgöz, M.A.; Arunasalam, A.; Halim, M.A.H.A.; Shamsudin, Z.B.; Kumar, S.; Sinniahet, A. Local trends of antibiotic prescriptions for necrotizing fasciitis patients in two tertiary care hospitals in central malaysia. Antibiotics 2021, 10, 1120. [Google Scholar] [CrossRef]
- Boutrot, M.; Azougagh, K.; Guinard, J.; Boulain, T.; Barbier, F. Antibiotics with activity against intestinal anaerobes and the hazard of acquired colonization with ceftriaxone-resistant Gram-negative pathogens in ICU patients: A propensity score-based analysis. J. Antimicrob. Chemother. 2019, 74, 3095–3103. [Google Scholar] [CrossRef]
- Gelaw, L.Y.; Bitew, A.A.; Gashey, E.M.; Ademe, M.N. Ceftriaxone resistance among patients at GAMBY teaching general hospital. Sci. Rep. 2022, 12, 12000. [Google Scholar] [CrossRef] [PubMed]
- Tewabe, A.; Marew, T.; Birhanu, G. The Contribution of nano-based strategies in overcoming ceftriaxone resistance: A literature review. Pharmacol. Res. Perspect. 2021, 9, e00849. [Google Scholar] [CrossRef]
- Yahav, D.; Duskin-Bitan, H.; Eliakim-Raz, N.; Ben-Zvi, H.; Shaked, H.; Goldberg, E.; Bishara, J. Monomicrobial necrotizing fasciitis in a single center: The emergence of Gram-negative bacteria as a common pathogen. Int. J. Infect. Dis. 2014, 28, 13–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahim, G.R.; Gupta, N.; Maheshwari, P.; Singh, M.P. Monomicrobial Klebsiella pneumoniae necrotizing fasciitis: An emerging life-threatening entity. Clin. Microbiol. Infect. 2019, 25, 316–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.Y.; Yu, S.N.; Lee, E.J.; Kim, T.; Jeon, M.H.; Choo, E.J.; Park, S.; Chae, J.W.; Bang, H.I.; Kim, T.H. Monomicrobial gram-negative necrotizing fasciitis: An uncommon but fatal syndrome. Diagn. Microbiol. Infect. Dis. 2019, 94, 183–187. [Google Scholar] [CrossRef]
- Huang, T.Y.; Peng, K.T.; Hsiao, C.T.; Fann, W.C.; Tsai, Y.H.; Li, Y.Y.; Hung, C.H.; Chuang, F.Y.; Hsu, W.H. Predictors for gram-negative monomicrobial necrotizing fasciitis in southern Taiwan. BMC. Infect. Dis. 2020, 20, 60. [Google Scholar] [CrossRef] [Green Version]
- Timsit, J.F.; Ruppe, E.; Barbier, F.; Tabah, A.; Bassetti, M. Bloodstream infections in critically ill patients: An expert statement. Intensive. Care Med. 2020, 46, 266–284. [Google Scholar] [CrossRef] [PubMed]
- Wong, G.; Taccone, F.; Villois, P.; Villois, P.; Scheetz, M.H.; Rhodes, N.J.; Briscoe, S.; McWhinney, B.; Nunez-Nunez, M.; Ungerer, J.; et al. β-Lactam pharmacodynamics in gram-negative bloodstream infections in the critically ill. J. Antimicrob. Chemother. 2020, 75, 429–433. [Google Scholar] [CrossRef] [PubMed]
- Duncan, C.J.A.; Barr, D.A.; Seaton, R.A. Outpatient parenteral antimicrobial therapy with ceftriaxone, a review. Int. J. Clin. Pharm. 2012, 34, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Kamfose, M.M.; Muriithi, F.G.; Knight, T.; Lasserson, D.; Hayward, G. Intravenous ceftriaxone versus multiple dosing regimes of intravenous anti-staphylococcal antibiotics for methicillin-susceptible Staphylococcus aureus (MSSA): A systematic review. Antibiotics 2020, 9, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alsowaida, Y.S.; Saleh, Y.; Benitez, G.; Saleh, K.B.; Almangour, T.A.; Shehadeh, F.; Mylonakis, E. Effectiveness and safety of ceftriaxone compared to standard of care for treatment of bloodstream infections due to Methicillin-susceptible Staphylococcus aureus: A systematic review and meta-analysis. Antibiotics 2022, 11, 375. [Google Scholar] [CrossRef]
- Yetmar, Z.A.; Razi, S.; Nayfeh, T.; Gerberi, D.J.; Mahmood, M.; Abu Saleh, O.M. Ceftriaxone versus antistaphylococcal antibiotics for definitive treatment of methicillin-susceptible Staphylococcus aureus infections: A systematic review and meta-analysis. Int. J. Antimicrob. Agents 2022, 59, 106486. [Google Scholar] [CrossRef] [PubMed]
- Hirai, Y. Treatment options for gram-positive and gram-negative bacteria: Focus on ceftriaxone. Clin. Med. Rev. Ther. 2011, 3, 215–234. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| No. of | Hemorrhagic | Nonhemorrhagic | Bacteremia | Mortality | |
|---|---|---|---|---|---|
| Variable | Patients | Bullae | Skin Lesions | ||
| Monomicrobial Infection | 74 | 50 | 24 | 39 | 6 (8.1%) |
| Gram-positive pathogens | 22 | 7 | 15 | 0 | 0 (0%) |
| MRSA | 5 | 4 | 1 | 0 | 0 |
| MSSA | 10 | 2 | 8 | 0 | 0 |
| Streptococcusdysgalactiae | 4 | 1 | 3 | 0 | 0 |
| Corynebacterium falsenii | 1 | 0 | 1 | 0 | 0 |
| Staphylococcus epidermidis | 1 | 0 | 1 | 0 | 0 |
| Bacillus | 1 | 0 | 1 | 0 | 0 |
| Gram-negative pathogens | 52 | 43 | 9 | 39 | 6 (11.5%) |
| Vibrio vulnificus | 40 | 32 | 8 | 31 | 3 |
| Vibrio cholerae non-O1 | 1 | 1 | 0 | 0 | 1 |
| Vibrio parahemolytics | 1 | 1 | 0 | 1 | 0 |
| Aeromonas hydrophila | 4 | 4 | 0 | 1 | 1 |
| Aeromonas sobria | 1 | 1 | 0 | 1 | 0 |
| Klebsiella pneumonia | 2 | 1 | 1 | 2 | 1 |
| Serratia marcescens | 1 | 1 | 0 | 1 | 0 |
| Escherichia coli | 1 | 1 | 0 | 1 | 0 |
| Achromobacter xylosoxidans | 1 | 1 | 0 | 1 | 0 |
| Polymicrobial Infection | 6 | 5 | 1 | 1 | 0 (0%) |
| No growth | 29 | 5 | 24 | 0 | 2 (6.9%) |
| Total | 109 | 60 | 49 | 40 | 8 (7.3%) |
| No. of | Ceftriaxone- | Ceftriaxone- | Other Antibiotic- | |
|---|---|---|---|---|
| Variable | Patients | Susceptible | Resistant | Resistant |
| Gram-positive pathogens | 22 | 16 | 6 | |
| MRSA | 5 | 0 | 5 | OXA, AMP, ERY, CLI |
| MSSA | 10 | 10 | 0 | ERY, PEN |
| Streptococcus dysgalactiae | 4 | 4 | 0 | CLI, ERY |
| Corynebacterium falsenii | 1 | 0 | 1 | CAP, ERY, CIP |
| Staphylococcus epidermidis | 1 | 1 | 0 | OXA, PEN |
| Bacillus | 1 | 0 | 1 | PEN, TRC, ERY, AMP |
| Gram-negative pathogens | 52 | 51 | 1 | |
| Vibrio vulnificus | 40 | 40 | 0 | None |
| Vibrio cholerae non-O1 | 1 | 1 | 0 | AMP, CAP, SMX–TMP, TRC |
| Vibrio parahemolytics | 1 | 1 | 0 | CFU, CEZ, CIP |
| Aeromonas hydrophila | 4 | 4 | 0 | ERT, TRC |
| Aeromonas sobria | 1 | 1 | 0 | ERT, TRC |
| Klebsiella pneumonia | 2 | 2 | 0 | None |
| Serratia marcescens | 1 | 1 | 0 | CFU, CEZ |
| Escherichia coli | 1 | 1 | 0 | None |
| Achromobacter xylosoxidans | 1 | 0 | 1 | AMK, CIP, CEF, GM |
| Total | 74 | 66 | 6 |
| Gram-Negative Group (N = 52) | Gram-Positive Group (N = 22) | p Value | ||
|---|---|---|---|---|
| Age (years) | 69.7 | 64.5 | ||
| Sex | ||||
| Male | 38 | 15 | ||
| Female | 14 | 7 | ||
| Mortality rate (%) | 11.5 | 0 | ||
| Deaths | 6 | 0 | ||
| Survivals | 46 | 22 | ||
| Positive culture | ||||
| Wound | 13 | 22 | ||
| Blood | 17 | 0 | ||
| Wound and blood | 22 | 0 | ||
| Isolates of ceftriaxone susceptible | 51 | 15 | ||
| Presentation of bacteremia | 39 | 0 | 0.0001 * | |
| Death | 5 | 0 | ||
| Presentation of hemorrhagic bullae a | 43 | 7 | 0.0001 * | |
| Death | 6 | 0 | ||
| Survivals | 37 | 7 | ||
| Systolic blood pressure (mm Hg) a | 0.0004 * | |||
| ≦90 | 19 | 0 | ||
| >90 | 33 | 22 | ||
| Body temperature (°C) a | 0.023 * | |||
| >38.5 | 19 | 2 | ||
| <38.5 | 33 | 20 | ||
| White blood cell | Mean | 13,528.8 ± 8497.7 | 16,195.4 ± 6614.1 | 0.19 |
| counts (cells/mm3) b | ||||
| Band forms (%) b | Mean | 8.3 ± 9.8 | 3.6 ± 6.4 | 0.04 * |
| 0 | 9 | 9 | 0.0406 *a | |
| >0 | 43 | 13 | ||
| Segmented forms (%) b | Mean | 76.8 ± 14.7 | 84.3 ± 7.9 | 0.026 * |
| ≦74 | 17 | 2 | 0.0425 *a | |
| >74 | 35 | 20 | ||
| Lymphocyte forms (%) b | Mean | 8.1 ± 6.0 | 6.3 ± 4.4 | 0.19 |
| Platelet counts (per mm3) b | Mean | 134,815 ± 72,698 | 247,636 ± 154,001 | 0.0001 * |
| ≦150,000 | 26 | 6 | 0.08 a | |
| >150,000 | 26 | 16 | ||
| Albumin (g/dL) b | Mean | 3.49 ± 0.68 | 3.71 ± 0.49 | 0.16 |
| Odds Ratio | p Value a | |
|---|---|---|
| Variable | (95% Confidence Interval) † | |
| Bacteremia | 131.667 (7.461–2321.745) | 0.0009 * |
| Hemorrhagic bullae | 10.238 (3.244–32.314.925) | 0.0001 * |
| Systolic blood pressure ≦ 90 mmHg | 26.194 (1.504–456.271) | 0.0251 * |
| Body temperature > 38.5 | 5.758 (1.211–27.381) | 0.0278 * |
| Band forms > 0% | 0.302 (0.099–0.920) | 0.0351 * |
| Segmented forms ≦ 74% | 4.857 (1.016–23.226) | 0.0477 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, H.-Y.; Huang, T.-Y.; Chen, J.-L.; Kuo, L.-T.; Huang, K.-C.; Tsai, Y.-H. Rational Use of Ceftriaxone in Necrotizing Fasciitis and Mortality Associated with Bloodstream Infection and Hemorrhagic Bullous Lesions. Antibiotics 2022, 11, 1454. https://doi.org/10.3390/antibiotics11111454
Chen H-Y, Huang T-Y, Chen J-L, Kuo L-T, Huang K-C, Tsai Y-H. Rational Use of Ceftriaxone in Necrotizing Fasciitis and Mortality Associated with Bloodstream Infection and Hemorrhagic Bullous Lesions. Antibiotics. 2022; 11(11):1454. https://doi.org/10.3390/antibiotics11111454
Chicago/Turabian StyleChen, Hung-Yen, Tsung-Yu Huang, Jiun-Liang Chen, Liang-Tseng Kuo, Kuo-Chin Huang, and Yao-Hung Tsai. 2022. "Rational Use of Ceftriaxone in Necrotizing Fasciitis and Mortality Associated with Bloodstream Infection and Hemorrhagic Bullous Lesions" Antibiotics 11, no. 11: 1454. https://doi.org/10.3390/antibiotics11111454